Jul 7, 2020
Our Duty to Treat Opioid Use Disorder in Corrections
By Brent Gibson, MD, MPH, CCHP-P
Chief Health Officer, NCCHC
On June 22, NCCHC held an incredible webinar with national experts on the treatment of opioid addiction in correctional facilities. While the audience was largely clinicians, our talk was not intended to be technical because I can’t emphasize enough how important it is for any leader in correctional health care (or corrections in general) to have a handle on the basics of treating people addicted to opioids.
Important takeaway points include:
- Every incarcerated person deserves access to all FDA-approved medications for treatment of opioid use disorder (provided in an environment of comprehensive services, including behavioral health)
- Anyone choosing to practice in a correctional setting has a duty to learn how to treat these patients with standard-of-care medicine or how to immediately access these services
- Correctional leaders have a duty to provide the environment and the means that providers need to provide appropriate patient care and fulfill their professional and ethical obligations to their patients.
These together are critical to access to constitutional health care—patients are seen by qualified health care professionals, are rendered a clinical judgment, and receive care that is ordered—a founding value of the National Commission.
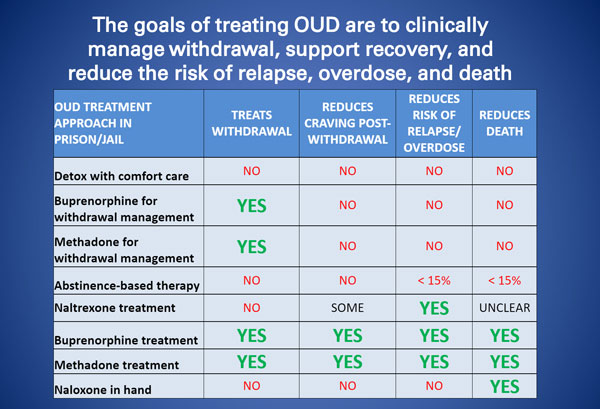
Inadequate Approaches
Regrettably, when working in the field and speaking with my colleagues across the nation, I have become aware that misunderstanding of the basics, among clinical and nonclinical professionals alike, leads to substandard care. This problem is widespread. For example, some believe that offering one or some medications (but not all) constitutes an adequate medication-assisted treatment program, others feel that providing agonist treatments to lessen the symptoms of withdrawal is sufficient, and yet others believe that antagonist treatment can be used as a stand-alone approach to treatment. There are also the extremes that behavioral health treatment alone or medication alone will suffice to treat patients suffering from this complex disorder.
Another problem I see is best described as making comprehensive treatment (including medications) available only to certain classifications of patients, such as pregnant women. Finally, for reasons that are not clear clinically, programs will continue medication that was administered in the community but will not attempt to treat OUD sufferers who are not in a current treatment program. I have also seen cases where security concerns lead to discontinuation of comprehensive care, without development of viable alternatives, a practice that smacks of health care being used as a punitive measure.
None of the things I have described is acceptable nor constitute adequate health care in a correctional setting. Solutions must be immediately developed. There is so much at stake and solutions are within reach of any correctional program. Expensive or complicated approaches are not required. What is required is commitment, focus, and follow-through.
If you have not viewed our webinar, I strongly urge you to do so now. The lives of your patients depend on it.